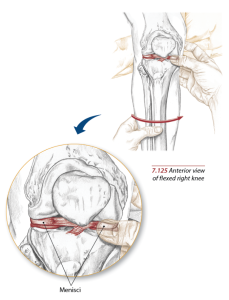
The meniscus, also known as the “shock absorber” cartilage of the knee, provides stability and cushioning to the knee joint. It consists of two C-shaped tissues, one on the inner (medial) side and the other on the outside (lateral) of the knee, and together they provide necessary cushioning between the shin and the thigh. Once damaged, can clients ever expect a properly functioning knee joint? Read on to learn about the multitude of considerations.
Causes of a Meniscus Tear
 Any activity that involves forcefully twisting the knee, either rotationally or with a shearing force across the tibiofemoral joint while it bears weight, can tear a meniscus. Performing squats with a very heavy load can cause such tears, as can any sports-related motion requiring an immediate directional change or a quick increase/decrease of movement patterns. Any traumatic impact to the knee can also result in damage to the delicate knee cartilage.
Any activity that involves forcefully twisting the knee, either rotationally or with a shearing force across the tibiofemoral joint while it bears weight, can tear a meniscus. Performing squats with a very heavy load can cause such tears, as can any sports-related motion requiring an immediate directional change or a quick increase/decrease of movement patterns. Any traumatic impact to the knee can also result in damage to the delicate knee cartilage.
Individuals who already display any degree of degeneration, most likely brought on by concurrent osteoarthritis, find that lesser forces can elicit meniscus tears. Physicians typically encounter this scenario in patients over the age of 40. In senior adults, age-appropriate degenerative changes in the knee can lead to a torn meniscus even in the absence of the aforementioned torque or impact.
Studies tallied in this country reveal a 61 per 100,000 incidence rate of meniscal tear injuries throughout the general population. Engaging in recreational/professional sports such as soccer, football, basketball, skiing, and wrestling poses an even higher risk of meniscal tears.
[sc name=”anatomy” ][/sc]
Recognizing an Injury
A torn meniscus causes pain, swelling, and stiffness. Some individuals report a “locking” sensation, as well as a reduced ability to move the knee through its full bending range of motion. In more severe tears, attempting to bear weight on the affected leg might prove extremely painful or impossible.
While in some cases, a mildly torn meniscus may respond well to R.I.C.E. (rest, ice, compression and elevation) and possibly over-the-counter NSAID’s, more serious tears could require surgical repair. Much of this decision rides on the type/specific location of tear and the amount of blood flow to that area.
Potential Tears and Treatment Options
Orthopedic surgeons encounter many variations on a torn meniscus; treatment usually depends upon the type/severity of the injury.
Incomplete tears or intrasubstance tears tend to occur in one’s 20’s or 30’s.
Such tears might point to early degenerative changes of the meniscus, simply the result of wear and tear, or overuse.
Radial tears represent the majority of all meniscus damage, appearing in an avascular zone of the meniscus, or an area with little to no direct blood supply. As we can imagine, a lack of blood flow prevents effective healing. The surgical option involves removal/cleaning out of the damaged part of the meniscus.
Horizontal tears occur along the curved fibers of the meniscus. In many cases, a surgeon can simply sew this type of tear together, depending upon where the damage occurred. If located within the vascular portion of the meniscus, by the outer side of the meniscus with ample blood flow, repair typically yields successful results.
A flap tear occurs when a portion of the cartilage gets peeled back and “stuck” in the joint. Such a tear causes the patient to feel a “catch” in his knee. Again, a surgical fix can eliminate this problem, without the need to remove very much surrounding tissue.
A bucket-handle tear, one of the more common horizontal tears, actually will prevent full range of motion throughout the knee joint. In these tears, surgical repair takes on a greater sense of urgency, since this offers the only way in which to allow the knee to once again bend fully.
To Repair or Remove?
Orthopedic surgeons can choose from two basic surgical approaches when treating a torn meniscus:
- Removal of the torn part of the meniscus, known as a meniscectomy
- Simply repairing the meniscus by reattaching the torn parts.
Both surgeries make use of a minimally-invasive approach called arthroscopy, in which two tiny incisions made in the knee – for the insertion of surgical instruments –means a faster recovery and less damage to the surrounding tissues.
When at all possible, physicians tend to opt for repair over meniscus removal. Many studies have shown that preserving the meniscus leads to better healing and long-term joint function. A 2019 study published in the American Journal of Sports Medicine involved 45 patients, all of whom presented with meniscus tears. 15 received non-operative treatments, 15 required the removal of a portion of the meniscus, and 15 underwent meniscus repair. Results indicated that those patients who had the repair procedure not only experienced less arthritis later in life, but also showed less likelihood to need a total knee replacement down the road.
Once a good portion of one’s meniscus gets removed, the knee joint receives considerably less cushioning, therefore exacerbating force transmission across articular cartilage. This most likely explains an increased tendency toward knee replacement in later years. In fact, research indicates that patients undergoing arthroscopic knee surgery resulting in a meniscectomy show a three -to four-fold increase in the risk for future knee replacement surgery.
Take-home Message
While many more long-term studies need to take place before physicians can definitively prove this conjecture, many believe a successful meniscus repair leads to more evenly spread stress upon the knee joint. Projecting even further, eliminating or reducing chances of uneven force might attenuate any risk of joint complications down the road. Take care and precautions when programming to protect the knee joints.
When clients mention knee discomfort or range of motion loss during a training session, personal trainers might do well to mention the possibility of a meniscus tear, and either suggest the client seek out an orthopedic knee specialist or significantly modify his workout to accommodate a vulnerable knee joint.
References:
https://www.sciencedirect.com/science/article/pii/S1877056817303286
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5800955/
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7914628/
https://www.verywellhealth.com/types-of-meniscus-tears-3862073
https://www.verywellhealth.com/eges-test-detecting-a-meniscus-tear-2549648
https://www.ncbi.nlm.nih.gov/books/NBK431067/
https://pubmed.ncbi.nlm.nih.gov/27712957/
https://www.mdedge.com/rheumatology/article/189316/osteoarthritis/total-knee-replacement-risk-soars-after-arthroscopic
https://www.uofmhealth.org/health-library/te7366
https://www.mayoclinic.org/diseases-conditions/torn-meniscus/symptoms-causes/syc-20354818
https://journals.sagepub.com/doi/full/10.1177/0363546519888212
Cathleen Kronemer is an NFPT CEC writer and a member of the NFPT Certification Council Board. Cathleen is an AFAA-Certified Group Exercise Instructor, NSCA-Certified Personal Trainer, ACE-Certified Health Coach, former competitive bodybuilder and freelance writer. She is employed at the Jewish Community Center in St. Louis, MO. Cathleen has been involved in the fitness industry for over three decades. Feel free to contact her at trainhard@kronemer.com. She welcomes your feedback and your comments!
