Many fitness enthusiasts in the course of their fitness journey eventually end up cursing everything from knees to toes. These bones, joints, and other tissues, both big and small, seem to be among those that are easiest to injure as a result of the repetitive forces we make them endure. Let’s break down the joints of the lower leg that we love to hate so much—what their normal function looks like and some likely causes of their dysfunction.
Let’s start at the most superior point and one of the two large joints of the lower leg we’ll be discussing: the knee.
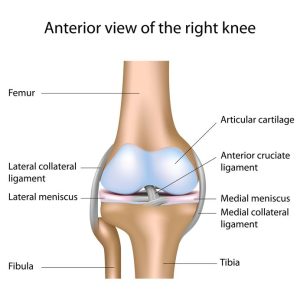 The Knee
The Knee
This joint is where the tibia, the smaller fibula, and femur converge. What we often think of as the primary portion of the knee- the cap or patella– is a minor player in this major joint. The cap’s main job is to protect the junction between three other bones and many ligaments that hold them together. Under the cap, there are two crucial ligaments known as the anterior and posterior cruciate ligaments. These ligaments are what attach your femur to the bones of your lower leg.
There are also another two ligaments that play an important part in this job as well: the medial and lateral collateral ligaments attaching to the various bones from all sides and providing the most strength possible for the knee.
The final major players in the knee joint are the menisci. These crescent-shaped, thick and relatively flexible cartilages are cushioning junctions between the femur and the tib/fib complex of the lower leg.
Common injuries to the knee revolve around two types of tissue: ligaments and cartilage. We have probably all known someone that has had ACL repair surgery. Damage to the ligaments is most often done by either direct blows to the knee causing hyperextension, or unnatural torsional forces being applied that stretch and damage the ligaments. Bear in mind that the knee is a hinge joint and only supposed to move in the sagittal plane (for the most part); a movement in another plane may likely cause an injury.
Injuries to the meniscus are most often a result of direct impact or, conversely, the action of the normal force on the feet. This observation is from where we draw the direct correlation between weight-loss and a reduction in meniscal injuries. The more force that is applied to this cartilage (which also acts on the femur under a normal force) results in a multiplicative relationship. Meaning, the less force we apply is also multiplicative in injury reduction.
Weight loss is a great way to protect your menisci and keep your knees cushiony for many years to come.
Moving distally down the leg we encounter the tibia and fibula. These two bones work synergistically to support the femur and, hence, the rest of our body. The tibia can specifically take a beating from repetitive impact activities like running, jumping, or maybe even something like kickboxing. This bone bears most of the weight of the human body.
The fibula does not do as much of the weight-bearing, but it is still important.It acts as the origin for many of the muscles of the thigh and hip that help us walk, and it also provides support for the ankle. We will review these muscles in later article as a part of this series.
 The Ankle
The Ankle
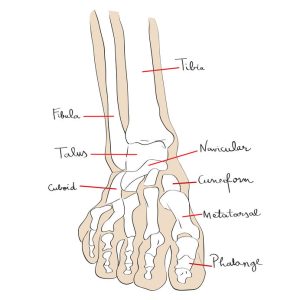
The fibula terminates at the malleolus—a bone of the lateral ankle where it connects to various bones by a series of ligaments. This attachment point allows for some additional stability within our ankle. The Achilles tendon runs from the calf muscles, the gastrocnemius and the soleus, to the posterior calcaneus (heel bone), and assists in plantarflexion.
This is where the simplicity stops, so in order to overt complexity going forward, we will address overarching concepts and categories of support rather than individual ligaments that make up these joints. Very similar to the knee, the ankle is supported and held in place by a set of ligaments referred to as the lateral and medial collateral ligaments. These ligaments provide support in a similar way to the lateral and medial cruciate ligaments of the knee, but with some more freedom in the range of motion.
From here, the ankle connects to the phalanges of the foot by ligaments that begin at the epiphyses of the ankle, or the most distal section of the tibia.
If you’re interested in the ligamentous anatomy of the ankle, please see this National Institute of Health article which includes a pictorial essay from a gross anatomy dissection of the ankle! It is quite interesting and goes much further in-depth than this blog article.
A Final Note
While we do not go into the gym every day planning to train the anterior cruciating ligament, weight training impacts our ligaments by encouraging them to grow stronger. Ultimately, this will be an important piece for maintaining stronger joints as we age and limiting injuries in the long run. Compared to muscle, it can take nine months or more of training in order to see some ligamentous improvement as a result of the lower limb vascularization, but it is so worth it!
Give the references listed below a closer look for a more in-depth explanation of ligaments and ankles.
References:
“Is Weight Loss Associated with Less Progression of Changes in Knee Articular Cartilage among Obese and Overweight Patients as Assessed with MR Imaging over 48 Months? Data from the Osteoarthritis Initiative” https://pubs.rsna.org/doi/10.1148/radiol.2017161005 by Alexandra S. Gersing , Benedikt J. Schwaiger, Michael C. Nevitt, Gabby B. Joseph, Nattagan Chanchek, Julio B. Guimaraes, John Mbapte Wamba, Luca Facchetti, Charles E. McCulloch, Thomas M. Link
Golanó P, Vega J, de Leeuw PA, et al. Anatomy of the ankle ligaments: a pictorial essay. Knee Surg Sports Traumatol Arthrosc. 2010;18(5):557-569. doi:10.1007/s00167-010-1100-x https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2855022/
Yang G, Rothrauff BB, Tuan RS. Tendon and ligament regeneration and repair: clinical relevance and developmental paradigm. Birth Defects Res C Embryo Today. 2013;99(3):203-222. doi:10.1002/bdrc.21041 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4041869/
