As a woman and personal trainer, I have both “suffered” with and fielded countless questions about cellulite. If you serve any women in your practice, I guarantee this topic will arise at some point and you should be prepared to handle both the scientific explanation of cellulite and also the discontent frequently associated with it. Here’s everything you need to know about cellulite and how to best inform your clients.
What is Cellulite?
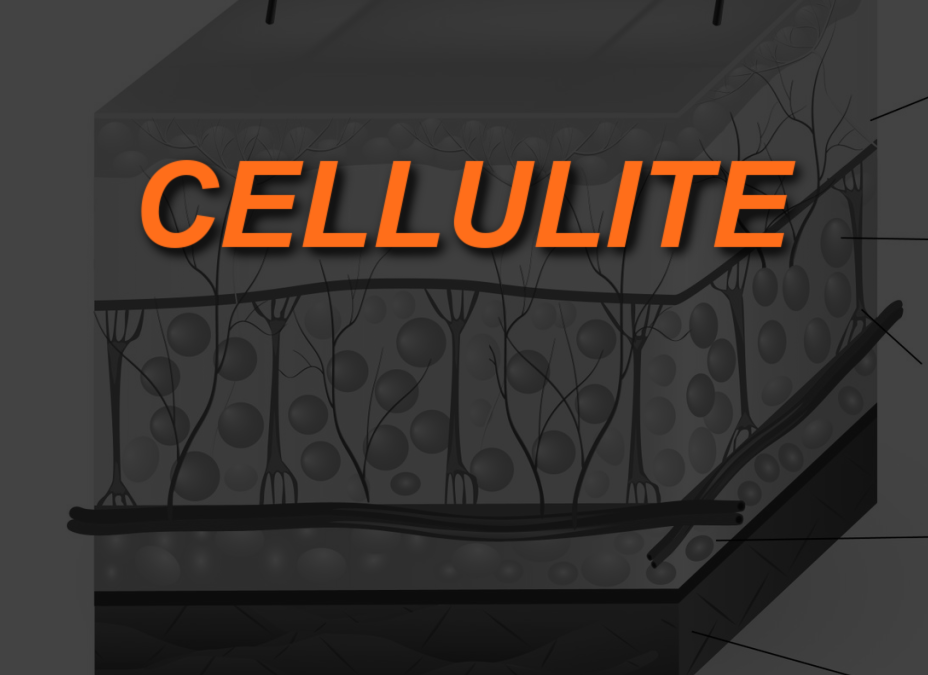
To tackle the issue of this fatty-fibrous phenomenon, one must understand exactly what it is without taking guesses based on appearance. Cellulite is the appearance of dimpling and puckering of the skin, most commonly affecting women (up to 90% of them!), and most likely to be found around the thighs, buttocks, and abdomen. The scientific designation, edematous fibrosclerotic panniculopathy, was first coined by Alquin and Pavot in 1920. They described cellulite as “interstitial edema associated with an increase in fat content.”1
In layperson’s terms, cellulite is a herniation of subcutaneous fat tissue from their fibrous collagen enclosures, which then creates the phenotypical appearance of skin depressions. The perpendicular nature of the fibrous septa in women is what ultimately manifests in the puckering. Men, on the contrary, have a transverse, or criss-cross, orientation of these connective tissue fibers, preventing the appearance of cellulite.
Unfortunately, the exact etiology of this complex condition is not clearly understood. There are several factors at play, and encouragingly, even some potential solutions to mitigate its appearance. While people of normal weight can still exhibit cellulite, the increased storage of fat cells will, in kind, exacerbate the appearance of dimpling.
In order to prevent the development of cellulite, lipogenesis (the development of adipocytes) must be slowed down while lipolysis, (the destruction of stored up fat), should be sped up.
Lifestyle Factors
Diet
We can say with certainty that excess adipose tissue will magnify the effects of cellulite, and so adopting a healthy lifestyle of nutritious foods and challenging activity will certainly reduce the amount of fat that can contribute to unsightly puckering. However, can the appearance of cellulite be reduced by specific dietary influences?
Some have proposed that an anti-inflammatory diet can reduce the puckered tissued appearance. This study concluded that a dietary intervention aimed at including fresh, preservative-free foods (whole grains, lean means, colorful fruit and veggies), free of added sugar, alcohol, pasta did not have an impact on visible cellulite despite some other markers improving (like skin thickness). The controlled diet did result in some weight loss, but it wasn’t significant. Further, the authors point out that “although there is no consistent evidence on which food groups affect cellulite, the analysis of the diet recall before the intervention showed that most participants were used to eating industrialized food, with high glycemic index and rich in trans fatty acids.”2
My personal take? I eat a very clean, and well-balanced diet of organic foods, minimal processing, and very low sugar. I do consume moderate alcohol, however. I have not found my cellulite to respond much at all to dietary interventions unless my body fat percentage decreased along with it. (and still, cellulite remains, just less prominent).
Smoking
Because if its deleterious effects on the cardiovascular system smoking is thought to increase the likelihood of cellulite. See the study below under “genetic influences”.
Hormones and Cellulite
The influence of hormones on the cardiovascular system cannot be ignored. The female hormone estrogen is abundant and women but still plays a role in the male endocrine system. Unfortunately, starting in puberty, women may develop an imbalance of estrogen and progesterone (another female hormone). The high ratio of estrogen to progesterone is known as estrogen dominance. Even if estrogen levels are too low, one can still be estrogen dominant, resulting in hormonal dysfunction.
Steroid hormones like estrogen are responsible for the dilation of blood vessels. While the manifestation of cellulite on the surface may appear to be limited to connective and adipose tissue, this is not the full picture. The circulatory and lymphatic systems are involved in the clearance of toxins and lipid metabolism. Without proper functioning, accumulation of fat will occur in subcutaneous tissue and toxins will happily reside there. Furthermore, over time, abnormal tissue perfusion and altered metabolism can weaken the walls of tissue that pucker and create cellulite.
This suggests that examining the balance of hormones may offer insight to not only the formation of adipose tissue and resulting cellulite, but other mysterious ailments and conditions that imbalanced hormones may cause. Seeking your body’s mineral balance and heavy metal load may shed significant light on what can be having an impact on hormones and the body’s detoxing pathways. This can be done through Hair Tissue Mineral Analysis. The results from this test offer a 2-3 month snapshot of the body’s heavy metal burden and mineral ratios that directly influence the body’s metabolic processess. Since women are higher in body fat, and since most of those that report cellulite are in fact women, getting a handle on the body’s hormone activity and metals that can be stored in fat tissue is a reasonable starting point to tackle this elusive condition.
Genetics
Like most things, science can point to some gene or polymorphism that explains, at least in part, why certain characteristics are expressed, and cellulite is no different. One experiment compared smoking and non-smoking women in their 30’s and whether or not they had a polymorphism of the ACE* gene (rs1799752/rs4343). Interestingly, women who smoked but did not have this polymorphism were less likely to exhibit cellulite. Meanwhile, women who did not smoke but did have the polymorphism were more likely to have visible dimpling. Finally, combine this specific polymorphism and smoking, and the women were almost 14 times more likely to have cellulite than women who did not have the mutation and did not smoke.3
*Note: The ACE gene controls blood pressure via expression of the ACE enzyme. With the DD (sometimes relayed as G,G) polymorphism you have higher ACE levels and higher chances of heart disease.
As a woman who has been athletic and enjoyed a low body fat percentage most of my life, yet have had visible cellulite on my thighs since I was 18, I found this piece very interesting. I went through my genetic health data and found that I do indeed have this polymorphism.
A second polymorphism was identified as increasing risk for cellulite expression, HIF1α.4 Though the association is not as strong as is with the ACE mutation, the presence of this allele is still significant. (I do not have this polymorphism). If this is you as well (and really, you don’t need to check your genetic data if you’re like me—the proof is in the pudding, no?).
What Can Be Done About Cellulite?
Are we to just accept that cellulite is part of our bodies and our life and just move on? The short answer is, yes. We should. Even if there are ways to minimize and eliminate cellulite (spoiler alert: I still haven’t been successful more than 20 years later), the number one thing we should do and encourage our clients to do is love and accept our flawed and imperfect bodies no matter what.
If I could rewind and tell my 20-something self that there are far more important things than aiming for bodily perfection I would have saved money, time, energy, and a healthy dose of self-deprecation. Self-love and body acceptance always paves the road to happiness, not self-loathing. The unattainable mission of bodily perfection is self-defeating (for most) and never-ending; once a fix is identified for cellulite your mind is likely to move on to the next “imperfection”, and so on and so forth.
Ultimately, if 90% of women exhibit the “ugliness” of fat-puckering somewhere on their bodies, it would follow that we are in very good company, and are still perfectly loveable. Full-stop. With that, there are still purported treatments, approaches, and procedures that may help to minimize the appearance of cellulite, which I will explore in the following article.
References
1. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6374708/
2. https://www.researchgate.net/publication/305731685_Does_A_Controlled_Diet_Improve_Cellulite
3. https://onlinelibrary.wiley.com/doi/abs/10.1111/j.1468-3083.2010.03827.x
4. https://onlinelibrary.wiley.com/doi/10.1111/j.1468-3083.2009.03556.x
As NFPT Blog Publisher from 2019 to 2024, and a veteran health and fitness trainer for over 20 years, Michele G Rogers, MA, NFPT-CPT, I-HTMAP, now serves as a Holistic Health Navigator and Practitioner, helping people improve their overall health utilizing Hair Tissue Mineral Analysis as a data-anchor. This functional medicine screening test enables clients to connect their physical symptoms to their emotional, cognitive, and spiritual health. She holds a master’s degree in applied health psychology from Northern Arizona University and multiple health certifications. Follow Michele on Instagram or find out more about her services at www.encompasspathways.com
