The shoulder is the most versatile joint of our body and allows motion of our arms in pretty much every direction, but this instability also makes it the riskiest joint. “What makes a joint risky?”, one may wonder. It is rather simple.
The increased range of motion requires a certain looseness and flexibility in the ligaments and tendons of the shoulder. This alone makes the shoulder more prone to injury, but the reckless abandon with which we can use our shoulders practically encourages it. While it is assured that the shoulder would be more stable with “tighter” tissues surrounding it- it would also be less useful if it behaved like a knee or elbow.
Shoulder Anatomy
Let’s talk about some of the things that make this joint different both in skeletal structure and musculature from other joints less likely to be injured.
How skeletal structure lends to shoulder instability
The glenohumeral (GH) joint makes up the ball and socket of the shoulder. This type of joint is exactly as it is sounds, observed as the humeral head (also known as the greater tubercle) attaching into the glenoid fossa. The GH articulation connects our arms to our torsos, and the shallow depth of the socket is part of what provides us with a significant range of motion.
A hinge joint on the other hand(like the knee or elbow) can only move (observably) in one plane of motion (flexion or extension), the shoulder is able to rotate, and abduct or adduct in addition to flexion and extension.
Another aspect to the GH joint to which we can ascribe more range of motion is the “capsule”: a series of fibers that encapsulate the joint and help provide some stability. This is not the only part of our anatomy that provides shoulder stability, however.
*The acromioclavicular (AC) joint and sternoclavicular (SC) joint also are involved in shoulder joint motions, but the focus here is on the instability of the GH joint.
How ligaments hold things together
The ligaments also do a large part of providing stability by attaching the bones to each other. This includes the coracoacromial, glenohumeral, and coracohumeral ligaments. As you may have guessed, each ligament is named for the bones to which it attaches: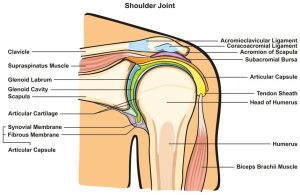
- The coracoacromial ligament attaches the coracoid process and the acromion to one another by a fibrous band
- The coracohumeral ligament attaches the coracoid and the humerus
- The glenohumeral ligament attaches the humerus directly to the glenoid. These ligaments serve to provide some basic stability in the posterior, anterior, and lateral directions.
More muscles involved can mean more risk for injury
Finally, the most responsive tissue in this region to training and unfortunately the most likely inducer of trauma- the muscles. There are eight muscles primarily involved in the movement of the GH joint, and can be categorized as either one of the four rotator cuff muscles or four global movers.
- The infraspinatus is a triangular band of a muscle that originates on the posterior face of each scapula on, running below the spine of the scapula. This muscle inserts onto the humeral head and performs external rotation of the arms. This muscle is antagonistic to the middle and posterior deltoids as well as the trapezius.
- The supraspinatus is named as such because it runs along the superior portion of the scapula in the supraspinous fossa and inserts into the greater tubercle. The positioning of this muscle allows us to abduct our arms (take them away from the midline of the body) almost primarily for the first 90 degrees. There are also some studies that indicate it may play the largest role in stabilization of the shoulder joint during lifting tasks. In consideration of this research, when our arms are in a resting position and gravity is the primary force acting upon them, pulling them down, it follows that a muscle attached to the top of the joint would play a significant role in supporting it.
- Teres minor originates on the lateral aspect of the scapula and runs up to the inferior portion of the greater tubercle. Shortening of this muscle results in external rotation of the arm, and it also aids in the stabilization of the humerus. It is antagonistic to the pectoralis major.
- Last, but not least, the subscapularis is a major player in our ability to pull and do rowing-type motions. It is deep, lying on the inferior surface of the scapula (beneath it, so “sub” scapular) and inserts into the lesser tubercle on the anterior aspect of the humerus. Like teres minor, this muscle is antagonistic to the pectoralis muscles as well; shortening allows internal rotation and adduction.
Global Movers
- Latissimus dorsi originate at the spinous processes of T7-L5 and insert in the intertubercular groove of the humerus (between the greater and lesser tubercles). It has a role in the adduction, extension, and internal rotation of our arms, as well as plays a major role in the rotation of the torso. It is antagonized by the deltoid and the trapezius muscles.
- Teres major is a short muscle that lies just beneath the lats, performing the same movements of adduction and internal rotation and supporting shoulder stability. Think of it as the lat’s little cousin.
- Pectoralis Major is situated on the chest, and while we do not normally think about it as a major shoulder mover, it plays an important role in horizontal adduction as well as balancing the tensions that act on the GH joint. This muscle is the anterior pull for the joint, and is antagonistic to the teres minor and subscapularis as well as other muscles of the upper back.
- The Deltoids are three band-like muscles that originate from the clavicle, spine, and acromion process and extend down the anterior, lateral, and posterior aspects of the humerus inserting into the deltoid tuberosity of the humerus. The difference in each of these bands is about where they begin. The anterior head originates in the clavicle, performing flexion and internal rotation by the shortening this band. The middle or lateral head originates at the acromion of the scapula, contributing to GH abduction, and the posterior head originates from the head of the scapula, which allows us to extend and laterally rotate our arms; it also performs horizontal abduction. Again, each head inserts into the same tuberosity, a lateral site of the humerus for the muscles to attach.
Pathology Contributing to Shoulder Instability
There are many things that can go wrong here but let us consider for a moment the one thing that is most often training-induced (as well as training-cured). The reason the antagonistic muscles were listed following a brief description of every major player in the GH joint is because antagonistic muscles are just as important to train (or avoid overtraining) as agonists. To avoid injury and postural dyskinesis, muscle imbalance must be prevented by giving equal weight to agonists and antagonists of each movement.
Dr. Arthur Pangmenan, with Pangmenan Chiropractic described a common issue specifically in men where the chest is overemphasized, and the result is to pull the shoulders in, creating a hunched appearance.
While this is not good for your appearance, it is also terrible for your shoulder functioning. It can compress the capsule along with nerve fibers and can even pinch muscles and ligaments. In short, it does not feel great and it does not result in quality movement.
Poor quality movements increase the likelihood of injury. Rather than being in stabilized equilibrium throughout your range of motion, you may have certain muscles that pull harder in one direction or another if they are overactive. Overactive, overdeveloped muscles will exert greater tension than the underactive ones, increasing risk for pulls and strains.
What A Trainer Can Do
A University of Washington Orthopedics and Sports Medicine article states, “In most positions the ball is held in the socket primarily by muscle action”. Training the muscles is one of the greatest things that can be done to increase stability. This means not ignoring the rotator cuff complex. Incorporate stability exercises as a warm-up before an upper-body workout, and keep an eye on form.
If your client demonstrates upper body dysfunction, then take the proper steps to help her resolve the muscle imbalances that are present before advancing in her training.
The next important thing to be done in training is to ensure equal tensions. Perhaps couple antagonistic muscles with their agonistic counterparts in your super-sets so that they get equal playing time? Or at the very least, make sure you program pulling as much as pushing. Be aware of disparities in strength and endurance.
Either way, ensure shoulder stability through equal training of all of the shoulder muscles to balance out their tension forces.
Another great benefit to training is that it will also increase the strength of your ligaments as well! They do not get tough quite as quick as muscular tissue but increasing their strength through resistance training will make the GH joint more resistant to dislocation and massive injury.
How have you prioritized shoulder stability in your client’s programming?
References:
Agonism and Antagonism of the Muscles of the Shoulder Joint
https://www.practicalpainmanagement.com/treatments/psychological/agonism-antagonism-muscles-shoulder-joint-semg-approach by Dr. Gabriel E. Sella, MD, PhD, MPH, MSc
About the Mechanics of Shoulder Stability
https://orthop.washington.edu/patient-care/articles/shoulder/about-the-mechanics-of-shoulder-stability.html
The Effect of Physical Activity on Ligamentous Strength: An Overview
https://www.jospt.org/doi/pdf/10.2519/jospt.1984.5.5.275 by Mark W. Cornwall, MS, PT, Barney F. Leveau, PhD, PT
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5731701/ Muscle Function in glenohumeral joint stability during lifting task by Yoann Blache, Mickaël Begon, Benjamin Michaud, Landry Desmoulins, Paul Allard, Fabien Dal Maso
https://www.ncbi.nlm.nih.gov/pubmed/12750133Dynamic Stabilizing function of the deltoid muscle in shoulders with anterior instability by Kido T1, Itoi E, Lee SB, Neale PG, An KN.
